In this section I will cover some helpful hints on how to accomodate the special
needs that sometimes come with hydrocephalus in the home. The brochure that
every parent gets on the day of the diagnosis that explains what
hydrocephalus is very good about explaining the mechanics of what is
happening in the brain, but it doesn't tell you a thing about what
you will need to do at home. The brochure that you get after the birth
that tells you what kind of shunt your child has and how to
be on the lookout for a shunt failure/infection also don't tell you
how to feed them or keep them safe while they are sleeping.
We were very lucky to have a great set of physical/occupational/speech
therapists in the hospital that helped us with all of this before we
went home. They also made sure that there was a physical therapist
waiting for us when we got home so that we could get settled in.
I highly recommend finding out if these services are available in
your hospital before the birth and getting them set up for home as
soon as possible after the child is born.
In this section I will share what we have learned through our
experiences, the experiences of other parents and suggestions from
therapists. We would love to hear any suggestions that other
parents might have so that we can include them here to share with
everyone. I certainly don't have all the answers, but hopefully
the info here will at least get the ideas flowing as to how
to settle in at home.
I also would like to note that I know that my son's head size is on the
extreme
end of how large a head can get. Most of the babies that I have met through
this site do not have heads as large as Owen's, so these things may or may
not be something you will need to deal with.
The biggest immediate worry that a parent has is the concern over a shunt
failure/infection. At first we were measuring Owen's head circumference a couple of times a
day. If it had gone up by even so much as a millimeter we started worrying and thinking about
heading for the emergency room. After all, the doctor had told us to watch for any change and
come in immediately if the size increased. Clearly he didn't realize that he was dealing with
two scientific types who would take this pretty literally.
We were driving ourselves crazy
with this until we finally asked the neurosurgeon exactly how much of a change was serious and
how long it would take for a change to occur. Having never seen a shunt failure, we didn't know
what to expect. He said that the head circumference can change a bit over time as the head grows,
and that even within a day it can go up and down a bit if the baby is more or less well hydrated.
The soft spot can also respond to hydration levels throughout the day.
The biggest thing
he said to watch for was the soft spot not sinking down some when you sit the baby completely
upright. It should drain and sink down a bit when you sit them up.
If it keeps sinking and
sinking and the baby fusses every time you sit them up, it could
be a sign of overdrainage. If you sit them up and it the soft spot is still bulging out
after a good period of time sitting up, then it might not be draining enough. Again, it's something
that you should wait a few hours and try again before really hitting the panic button because
sometimes it could just be a hydration thing.
A consistent change of head circumference of a half a centimeter in a
week, when it has been otherwise fairly stable, is significant enough to give the doctor a call.
A half a centimeter in a month is probably
just normal growth. Many times it will go up by a few millimeters for a few hours and then go
back down.
We did eventually experience a shunt failure, you can read about it
here. What we realized was that in
retrospect it was fairly dramatic. There were a lot of other signs that came with it too.
In our case it was a fairly slow decline in function and we saw some pooling of fluid and such
long before it failed enough to do something about. We also saw other symptoms such as
a lack of appetite and a general sleepiness. A baby may or may not exhibit any of these other
symptoms with a shunt failure, but the head circumference will almost always start going up. Once the
shunt failed completely it went up significantly - from 50 cm to 51 cm in about a week, but by the
time he actually had the surgery it had gone up to 52 cm in that last day or two. He started to
lose his appetite and started falling asleep every time you tried to feed him during that week of
fast growth. I also stand by the decision to go and have it checked out when fluid
started to build around the base of the shunt. Anything that out of the ordinary warrants a
trip to the doc.
We actually relaxed quite a bit after the shunt failure
because we realized that we will know pretty clearly when something is wrong. You do have
to keep an eye on things so that you catch it as soon as possible. We have just lowered the
panic level a bit. We now
measure his head circumference every other morning or so, more often if it seems a bit off.
We only start worrying when it has been up for a few days.
We do still keep a pretty close eye on the soft spot. It's pretty obvious when the shunt is
draining properly. It's probably the best indicator of what is going on.
Right from the beginning you should watch the bigger soft spot
towards the front of your baby's head and learn how it normally behaves. If you have a good
feel for how it behaves when things are working normally, it will be easier to see when
things are not working as they should.
For the first few weeks after he had the new shunt, and for the first few weeks after we brought
him home originally we took his temperature a couple of times a day to watch for infection.
Now we just keep an eye out when we give him a bath for any signs of redness along the
catheter tract and we watch for a temperature in the same way that you would for any baby, although
perhaps we are a bit quicker with the thermometer than we were with our daughter.
Another bit of info that the neurosurgeon shared with us is that the odds of a shunt failure
in an infant are pretty high. However, after the child is 1 year old the odds go down signficantly.
He also said that once a shunt has been in and functioning normally for a full 6 months the
odds of a failure also are greatly reduced.
Car Seat
The car seat is the first obstacle is getting your baby home. If you were able to
carry close to full term or your child's head is not that big then you may be able to use
a regular car seat. If your child is a preemie, or if the hospital has reason to believe
that he or she may not be able to support their own head sufficiently to get home safely,
they are required to do a car seat test. For this they have you bring in the car seat that
you plan to use for the trip home and they put the baby in the car seat, with a pulse/oxygen
monitor (aka a pulseox) on him, and they make them stay in the seat for the length of time that it will
take you to get home. So for us we had a three and a half hour drive. We were allowed
to take him out once an hour because we would be stopping once an hour on the way home. Owen
did not do well with his test. He had to struggle so much to keep his head up that he
set off his pulse alarm constantly. After only 15 minutes they took him out because he
just couldn't calm down. So we tried again the next day with the same results. It didn't
matter what the pulseox said, you could just tell by looking at him that he was scrunched
way down in the seat and could never do it for the whole drive home. We ended up ordering a
car bed
that worked out much better. It's nice and soft and he could just lay down in it. He ended
up using the car bed until he was about two months old and then he graduated to the regular
car seat.
When he finally moved up to a normal car seat, he still had trouble keeping
his head in the middle and would turn his head to the side and then fall
backwards. To help him with this we put a bendy bumper in the car seat
so that it holds his head. Without the bendy bumper he fights the whole
time he's in the seat to keep his head up. With the bendy bumper he
can rest and even sleep in the car seat.
If your child has a large head, you will need to keep them in a rear facing car seat
for longer than a normal child. Most of the traditional car seat/infant carriers with the
handle on them have a weight limit of only 20 to 22 pounds. The Graco SnugRide is
probably the most popular of these items and it goes up to 22 pounds, which is typically
just over a year old. The reason why infant car seats are rear facing is that an
infant's head size is very large as compared to the rest of their body. In a forward
facing seat that head would snap forward in a crash and cause serious damage. Most
children's bodies grow enough in the first year to make it so that their head is in
proportion to the rest of their body and they gain more head control. That
means that the weight of the head is
less likely to cause such damage in a crash and so you can turn them around to face forward.
Well our son was born with a head the size of a three year old's and it has grown some
since then because it doesn't seem to know that it doesn't need to bother. As such
his head is still way out of proportion to his body, but he weighs more than 22 pounds.
So we had to get him a new car seat that would allow him to stay rear facing. Strangely
enough, none of the "special needs" car seats are rear facing, which I find somewhat
surprising. So we started out with a Safety 1st All-in-One convertible car seat.
It had good reviews and was reasonably priced, but it was also a disaster. This
item is shown below:
As you might be able to see in the picture, there is a plate at the bottom of the
seat that is supposed to give back support, the entire back is fairly flat and
the sides don't come up very much. The plate and the flat back meant that it
didn't cradle him at all and he would fall over sideways, and since the sides don't
stick out very far he would hang out of the seat by the straps every time we
went around a corner. So we moved on to Plan B, which was the Britax Roundabout.
It cradled him very nicely and he could even sleep in it without slumping over.
This model is shown below:
It is more expensive than the Safety 1st model, but it was the only convertible
rear facing seat that looked like it would work. It's bigger brother the
Britax Marathon gets lots of rave reviews, but it would not fit in my Honda and
it didn't look like it would cradle him quite as much. The Roundabout is rear facing
up to 38 pounds and by the time he is that big he should be ready to face forward.
Sleeping Arrangements
There are three main issues to consider with sleeping arrangements for
young children with hydrocephalus:
The need to sleep at a high angle to drain CSF -
Almost all babies that have been shunted are required to be
kept at an angle for the first few weeks or months to help drain
the excess CSF. If your child has a relatively normal sized head
you can get away with a reflux pillow (just Google "reflux
wedge infant" and you'll find lots of companies that sell these).
If they have a larger head you might have to get more creative,
and you can see our solutions further down the page.
Needing to keep the airway open - Again, if your
child has a fairly normal sized head this probably won't be
a problem. But if your child has a large head that they cannot
control, it is possible that they will need some help to achieve this.
Our son's oxygen levels would drop while we were just holding
him, he was a preemie with a head the size of a three and a half
year old.
You can see our full solution below, but if you realize at the
hospital (where they are monitored constantly) that your child
has trouble with the weight of their head cutting off their
air flow, then at a minimum you will want to
keep the child on a pulse-ox (pulse/oxygen) meter at all times until
they are strong enough to keep this from happening.
Possibility of aspiration - If your child has a large
head that they cannot fully control, then they are at risk for
aspiration if they vomit while they are unattended in their crib.
This happened to us and you can read about it
here. Again your
best hope is monitoring. We had taken our son off all but the
sound monitors by the time this happened because he was
almost a year and a half old. While the sound
monitor did alert us that he was moving around, it is quite
obvious to us now that had we had the video or motion sensor
monitors on that we would have seen what was happening much sooner.
I can recommend two monitors that have had good luck with, and they
should stay on monitors until they have complete head control.
The first one is the Angelcare Movement Sensor - it has a pad
that you put under the mattress of the crib that senses the tiny
motions of a baby breathing. If the motion stops for more than 20
seconds, then it sounds an alarm. It comes with a remote piece that
you can carry with you that has a sound monitor on it that lets
you hear the baby, and the alarm if it goes off. This thing is
great - we used it for both kids and it works like a champ.
The second monitor is a handheld video monitor. We bought the
Summer Infant 900 MHz 2.5" Color Handheld video monitor. It has
a large enough range that I can see him clearly even when I'm
working outside. This has brought great peace of mind.
Our Sleeping Solutions
The doctors had told us that our son
needed to sleep at a 45 degree angle.
45 degrees is a very steep angle and with a big head on top and gravity wanting to pull everything
off that angle, it's a pretty hard thing to achieve. We also had the problem that
he could not keep his airway open with the weight of his head causing his neck to bend. While we were in the hospital Dora the
physical therapist made us one of these:
It was carved from a foam wedge. It's in it's naked form in the first picture, and you can
see that it has a big hole cut for his head, an indent cut for his body and a Bendy Bumper
(which you will find everywhere at the hospital) wrapped around it to keep him from sliding down.
The second picture is Owen sitting in his wedge (or baby barcalounger as we called it) in his
bed at the hospital. The hospital beds are nice because you can raise the bed to whatever angle
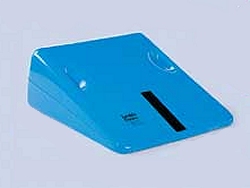
you want. When we got home I put it on one of the blue vinyl wedges shown in the third picture
with some pillows under the vinyl thingy to achieve the 45 degree angle. This setup was really
nice because it held his head and body in a perfect alignment so that his airway stayed open
and his body didn't get all scrunched up. This worked really well while he was fairly small.
When we got home we brought his wedge with us and put it in his crib,
but we also wanted him to be able to stay downstairs with us during the day.
We also wanted to allow him a greater freedom of movement than he could get in the carved out
wedge. So, I made him one of these:
It's a series of thin foam pieces, each one smaller than the one below it, glued together to
make a stair. On top of that is some blue orthopedic foam that Dora sent home with us, with
some other pieces of blue foam glued around the edges to make a bumper. The second picture
shows it covered with a blanket so that they don't sweat, spit up on, or pee on the foam.
It was really light so we could either put it on the floor with us or we could put it in the crib.
It also worked for him to sleep on at night when he outgrew the carved foam wedge. When
he started to roll down to the bottom as he got bigger, we made a V out of a Bendy Bumper (seen above)
to keep him from sliding down. When Owen was two months old the neurosurgeon gave us the
go-ahead to lay him down flat in the crib like a normal baby. If you are not feeling this
creative or simply want an easier way, we did see this
item
that we thought might have been just as good, if not better.
Another Mom used the
Carry-me-Near 5-in-1 Bassinet Sleep System by The First Years and she felt that
it made it easier to position her son than a full sized crib. If you don't already
have a crib from a previous child (as we did) then this might be a good thing to try
as there is a lot less space to fill in with pillows and wedges in a bassinet.
If anyone else has a suggestion on sleeping arrangements (or anything else),
email it to me and I'll be sure to include it.
Medical Equipment Rental
This is another one of those things that you don't realize
is available until you need it. I had my laptop with me while Owen was in the hospital and I
was looking online to buy a pulseox monitor, they are very expensive. These wonderful little things constantly monitor
the baby's blood oxygen level and it only uses a red light to do it.
While Owen was in the hospital this thing was my best friend.
It is not easy to hold a baby that has such a large head, and even when you are just sitting
with them in a chair, they eventually slump down ever so slowly until they are cutting off their
own oxygen supply and they aren't able to do anything about it. It's very scary and I was
afraid that when we got him home he'd slump down in his crib and we'd find him in the morning in
a lump down at the bottom of his wedge, not breathing. When I expressed this concern to the doctor
she said, that's easy, we'll just send you home with one. I explained that they were very expensive,
and she explained the wonders of medical equipment rental. They had a really nice one delivered to
my hospital room before we even left. It had a battery pack so that it could be used in the car on
our ride home. The insurance covers this as well. They also sent us home with a feeding pump
(which we never used), oxygen tanks and a suction machine. It felt like we were bringing half the
hospital home with us, but we also felt that we were ready to deal with anything that might come up.
Legal Disclaimer: While every effort has been made to make certain that the information contained in this website is accurate, it must be remembered that the content is managed by a parent, not by a doctor. Information contained here is for general support purposes only and is no substitute for the care of a physician.