Info - General Information About Congenital Hydrocephalus
This page contains general information about what congenital hydrocephalus
(also known as fetal hydrocephalus) is,
the diagnostic tests that are generally involved, the
treatment options that are available and some general steps that you can take to
make sure that you get the best information possible.
OK, your doctor most likely covered this when they gave you the diagnosis. There were a few
items that were missed during our initial discussions with the doctor though, most likely because
he realized that we weren't soaking in anything other than the fact that there was a problem.
So we'll cover the basics here. The short definition of hydrocephalus is as follows:
The brain is constantly producing fluid (known as cerebrospinal fluid or CSF) as part of
its normal daily routine. Under normal circumstances, this fluid is drained from the
brain into the spinal canal and is reabsorbed by the body, keeping the amount in the brain
in a constant balance. When normal drainage does not occur, or for some reason
the brain is producing too much CSF to be able to drain through normal means, the CSF builds up in the
ventricles of the brain and causes pressure. This condition is known as hydrocephalus
and, despite the fact that it is one of the single most common birth defects, most people have
never heard of it. Some types always develop early in the pregnancy, but other types
caused by bleeding or a tumor may not show up until later in the pregnancy.
That sounds pretty straightforward and isn't too hard to grasp. The problem comes in figuring
out why the hydrocephalus is occuring. It turns out that a great number of things can cause
that drainage to fail. Knowing something about why the fluid isn't draining can help
in determining the outcome for the baby.
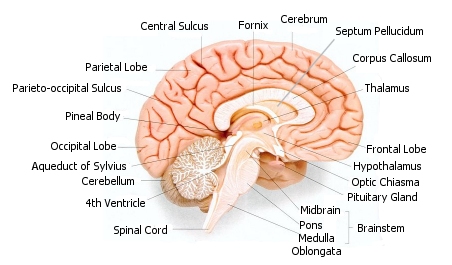
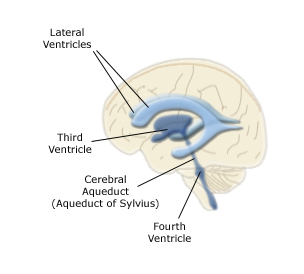
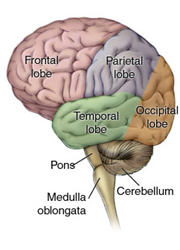
We have found out that there are several causes of fetal (congenital) hydrocephalus and they are described
below. To help you find some of the parts of the brain that are mentioned below, let's start out
with a few pictures:
Aqueductal Stenosis - This is the most common form of fetal
hydrocephalus, and it
is the form that our baby has. There is a narrow channel which connects the third and
fourth ventricles of the brain to allow CSF to drain. This channel is called the Aqueduct of Sylvius.
When this aqueduct is blocked, or was never properly formed, the CSF cannot drain properly and
this condition is called aqueductal stenosis. Blockage of the aqueduct can be
caused by a malformed aqueduct, a tumor,
swelling due to infection or intraventricular bleeding. This blockage results in
the enlargement of the ventricles. This type is generally not
caused by chromosomal abnormalities.
X-Linked Aqueductal Stenosis - I put this in its own category because while it is
caused by a blockage in the aqueduct, the reasons and associated outcomes are quite different.
In this case the cause is a mutation in the L1CAM gene on Xq28. No, I don't know
exactly what that means either, but I do know that it means that in addition to the problems
caused by the pressure, you can expect other types of problems as well that are caused by the
gene mutation. Many (but not all)
babies with this type have abducted thumbs. Abducted thumbs can often be seen
on an ultrasound and the doctor will probably look for this indicator
if a diagnosis of hydrocephalus has been made.
X-Linked Aqueductal Stenosis is an x-linked recessive condition. There are two
chromosomes that form a pair which determine gender in a person. For a boy the
pair is made up of one X and one Y chromosome. For a girl the pair contains two X's.
In order for a person to have a condition that is carried by a recessive chromosome,
both chromosomes in the pair must have the genetic mutation that causes the condition.
For this reason it is almost, but not quite, impossible for X-Linked Aqueductal Stenosis
to be passed on to a girl. X-linked conditions are carried only on the X chromosome,
and since boys only have one X chromosome, there is no second one to cancel it out.
Therefore if a boy has the mutation in their X chromosome, they will have X-Linked
Aqueductal Stenosis. A girl has two X chromosomes, which means that both would have
to have the mutation for the girl to have X-Linked Aqueductal Stenosis. Since the
mutation is extremely rare, the odds of having it in both the mother and father to pass
down to the girl to form a pair of mutated chromosomes are very, very small.
Chiari Malformations -
When the indented bony space at the lower rear of the skull, known as the posterior fossa, is smaller than
normal, the cerebellum and brainstem can be pushed downward. The resulting
pressure on the cerebellum can block the flow of cerebrospinal fluid causing hydrocephalus.
Normally the cerebellum, fourth ventricle and brainstem sit just above
the foramen magnum,
which is the opening in the bottom of the skull where the spinal cord attaches to the brainstem.
There are several different degrees of Chiari Malformations, depending on how far down the
cerebellum has been pushed.
Chiari I - where just a portion of the cerebellum has been pushed down
into the
spinal canal. A Chiari I may not have any symptoms, or may cause problems with balance,
dizziness, blurred vision, loss of muscle strength or spasticity.
Chiari II - In this type not only has the cerebellum been pushed downward into
the spinal canal, but
so has the fourth ventricle and the medulla (lower portion of the brainstem). This type is
generally associated with spina bifida (myelomeningocele) which is a condition where the
spinal cord does not close properly before birth.
Chiari III - Portions of the cerebellum and/or brainstem are pushed out
through a hole in the back or neck. This type has a high fetal and infant mortality rate,
and a high rate of severe complications in those that survive. The hole defect is closed
with surgery and a shunt is placed for the hydrocephalus. This form is very rare.
Chiari IV - An extremely rare form where the cerebellum does not fully form, and which
is rarely survived.
Dandy-Walker Malformation - Normally the cerebellum has two hemispheres which are separated
by a narrow structure called the vermis. A Dandy-Walker malformation is characterised by
a complete or partial absence of the vermis, along with a cyst located in the posterior fossa
(the indentation at the base of the skull). The cyst communicates, or transfers CSF back and
forth, with the fourth ventricle causing it to enlarge. There are other variations which can
mimic the appearance of a Dandy-Walker malformation, but do not have the agenesis (absence)
of the vermis of the cerebellum and the cyst does not open into the fourth ventricle. These variants are
much more benign and have a better prognosis. The prognosis for a child with a true Dandy-Walker
depends on the severity of the malformation and on whether or not there are other associated defects.
Dandy-Walker malformations are often found with other problems,
including agenesis of the corpus callosum and malformations of the face, limbs, fingers, toes and heart.
Trisomy Chromosomal Defects - Normally a human has 23 pairs of chromosomes, one set of 23 from
the mother and one set of 23 from the father. The pairs are numbered from 1 to 23. Trisomy
occurs when there are three chromosomes instead of just a pair of one of those numbered sets.
The most common are Trisomy 13, Trisomy 18 and Trisomy 21 (Down Syndrome) meaning that the 13th, 18th or
21st pair has an extra chromosome. Trisomies 13 and 18 are generally considered to be "inconsistent with life",
meaning that these children do not usually survive.
I mention these only because the perinatologist who gave
us our diagnosis
started out by telling us that there was an excellent chance that this is what we were dealing with.
I have no idea what he based that assumption on, but other parents have shared similar stories with
us, that their initial diagnosis came with the news that it was likely that their child had one of these
conditions and might very well not live. Based on this we, and other parents, told our other children
that their little brother or sister may not live. We now know that while it is a possible diagnosis, it
is not necessarily the likely diagnosis. An amnio will tell you for certain and these conditions are
the ones that show up on the FISH test in the first few days,
so don't worry about it until you get the results back.
Others - There are a number of other conditions that can also cause hydrocephalus
or are associated with hydrocephalus. Tumors and hemorrages are common causes of hydrocephalus.
Hydrocephalus is also sometime associated with agenesis of the corpus callosum -
where the membrane that divides the two hemispheres of
the brain does not form.
Anencephaly - where the brain fails to form
and fluid is all that is present is often incorrectly labeled as hydrocephalus.
While sometimes the hydrocephalus can exist in isolation, it also often appears
in conjuntion with a spectrum of other birth defects.
There are just so many things that fall under the umbrella of hydrocephalus that you can't
really
start thinking about what the diagnosis of hydrocephalus means for your baby until you can
determine something about the cause.
Treatment Options?
This is the part that really drove us crazy and was probably the single largest contributor to
the big hills and valleys in the roller coaster. If you read nothing else on this website,
read this section because it will save you the most pain.
In-utero surgery? Not in the USA! -
There are a number of articles out there
that are easily found on the web that describe in-utero surgery for hydrocephalus.
These
articles describe how shunting can be done while the baby is still in the womb and
show great excitement about the hope that this surgery brings. The catch? You can't
actually get this surgery anywhere in the USA. The most easily found articles are from
Vanderbilt University like
this one.
I called them to see if we could get the surgery and the nurses told me that it
couldn't be done anymore. I emailed one of the doctors that actually did
the surgery in the past and he emailed me back saying that no, they don't do the surgery anymore.
I spoke with doctors at the Children's Hospital of Philadelphia and the University of
California San Francisco Children's Hospital, which also do fetal surgery and they both also
said that the surgery was no longer available.
Surprisingly, the reasons given for why this surgery had been stopped were vague. They
mostly revolved around the idea that the risks were great and they couldn't really
prove that the outcomes were any better with the surgery than they were without it.
I have now read quite a few articles on the subject and I have found that most of the
risk seems to be with infection and malfunction of the shunt. There is also the problem
that hydrocephalus is often found with other conditions which don't always show up
on ultrasound or MRI that can complicate the outcome. You can find out the
results of the Vanderbilt study
here.
The subject is not entirely closed however. The research into prenatal surgery continues,
although mostly in other countries. You can read about one recent case study in
Saudi Arabia here.
Dr. Sergio Cavalheiro of the Universidade Federal de São Paulo in Brazil
has done a lot of research into this subject and has published some very promising
results. We actually pursued the idea of having him do the surgery on our son while
I was pregnant. I was able to contact him via email and at first he said that yes he could do the surgery and could I
please send down my records. When I asked him where to send the records and how much would the
surgery cost, he never replied. I'd like to think that he just went away on business somewhere
for a few months and couldn't reply, but several attempts at email were ignored. I don't speak
Portuguese, so I don't think I would have had much luck in contacting them via phone. A
person with better language skills and less of a fear of going to a country where they don't
speak the language for major/risky surgery might have better luck. You can read
one of Dr. Cavalhiero's articles here.
Shunting shortly after birth - This is pretty much your only option and is likely
to happen in all but the mildest cases. As described above, a shunt is basically a tube
that is placed in affected ventricle of the brain that has a valve on it to make sure the
fluid only flows out of the brain. The other end of the tube can be placed in various places
such as the heart or lungs, but most often it is placed in the peritoneal cavity, which is the
space surrounding the stomach. The peritoneal cavity is capable of absorbing large quantities
of fluid and can easily soak up whatever the brain puts out. A nice picture showing how a shunt
is placed can be found here.
Once the shunt is in place the fluid begins to drain and the ventricles (and therefore the head)
begin to shrink down to normal size. Our neurosurgeon says that this can be quite dramatic
and in a severe case like ours it is possible that the head circumference can shrink by as much as
7 to 8 centimeters (2.75 to 3.15 inches) in the first week. This didn't happen for us
as we only managed to go from 52 cm to 49.5 cm, but I have seen many babies where very
large heads have been brought way down in size.
Deliver the baby early - I am updating this entry now that Owen is a year old and
I am a year wiser. As you can read in our story, we were very gung-ho to have the birth
as early as possible. We had read many articles about how babies born at 32 weeks almost always
survive and it seemed that we should just get him out as soon as possible to put the shunt in
and take off the pressure. We urged our doctors to consider a birth at 32 weeks, or at the very
least at 34 weeks when the chances were even better. They all refused and said that we should
have the birth at 36 weeks. We fought very hard against this. Now I am glad that the doctors
stood their ground. As our neurosurgeon later told us, a normal baby that just has to survive
might be able to do that. However, babies with hydrocephalus have to not only lie there and breathe,
they have to survive brain surgery and general anesthesia within a day or two of birth. That is
a whole different ball game and requires a much stronger baby.
There is also the issue of the thickness of the skin. During the last few weeks in the womb, the
baby spends a lot of its time building up the layer of fat under the skin which adds thickness and
structure to the skin. Preemies are notorious for having thin skin, which mostly brings to mind
a problem with keeping warm. What it means to a baby with hydrocephalus though, is that it might
not be possible to place a shunt if the skin is too thin. Born at 35 weeks, (Owen's choice, not ours)
Owen's skin was still quite thin and it was quite a surgical feat to get the shunt in. You could
almost read the writing on the tubing through the skin. Below is a picture of Owen's shunt right
after it was put in, you can see the white tubing through the skin:
We had to be extremely careful that he didn't lay on it at all so that the skin didn't tear. They
forced as many calories into him as they could for the first few weeks to build up the skin around
that area. This all would cause us problems later because only the smallest tubing could be placed
under his thin skin and it started clogging within two months. If there is not enough skin to
put over the shunt, then an external ventricular drain has to be put in until a shunt
can be placed. Owen had a programmable shunt put in and these are larger than the
non-programmable kind. We were told before he was born that there was a chance that they
would not be able to place a programmable if there wasn't enough skin. The programmable
shunt has already saved him at least one and possibly two surgeries.
In addition to these problems, you also increase the risk of causing the problem that you are
trying to prevent: brain damage. If there are breathing difficulties which cause a lack of
oxygen for any length of time, then brain damage can occur. The earlier the child is born, the
greater the risk of this happening. You can also expect a longer stay in the hospital because
of feeding issues. Every case is different, of course, but I now understand why it is that they
were so adamant that we wait until at least 36 weeks. It's a balancing act between wanting to relieve the
pressure and avoiding causing more problems.
Cord Blood therapy - I found out via a newsletter from the Cord Blood Registry (where
we banked our daughter's cord blood) that some promising research is being done in using cord
blood stem cells to treat pediatric brain damage. (See
here
for one of the case studies). Through the wonders of Google and the
internet I was able to trace this research back to a Dr. Joanne Kurtzberg at Duke University
Medical Center. I got in touch with
Dr. Kurtzberg and she said that while the treatment had never been tried specifically for
hydrocephalus, that there was no real risk involved in the treatment and there was sufficient enough
promise in the treatment to make it worth the attempt. You can read more about this
on the cord blood page.
Endoscopic Third Ventriculostomy (ETV) - This treatment option is generally only for
cases of aqueductal stenosis where it is the third ventricle that fails to drain and it is
also not generally successful in newborns. This is actually a very old treatment that
involves putting a hole in the floor of the third ventricle to allow drainage without a shunt.
Newer techniques and technologies have greatly improved this option in recent years.
Our neurosurgeon says that this procedure is not generally successful in newborns
because they heal too well and often the hole just closes up. He did say that it will be an
option when our baby is at least a year old. It is not successful in all cases, but if it is
then the baby will not have a lifelong dependency on shunts which can malfunction or become infected.
You can find out more about this procedure
here. It should be
noted that this procedure also carries its own risks and is also something that must be
managed throughout a lifetime of checkups.
We have our diagnosis, what do we do now?
This is the hard part. I'm assuming that if you are at home reading this then you are
at least through the worst first few hours after diagnosis. Now what you need is a plan.
Get an amnio -
If your personal beliefs allow for it, the first thing to do is to get an amnio done.
We were dead set against an amnio when we
got pregnant. We didn't want to introduce risk into the pregnancy just for "peace of mind".
Well our perspective changed radically once we got a diagnosis like hydrocephalus.
The amnio can rule out most chromosomal problems. Some of the conditions that can
cause hydrocephalus are caused by chromosomal abnormalities such as Down Syndrome (also
known as Trisomy 21) or Trisomy 13 or 18 which are generally fatal. Our doctor told us right
away that these were a likely cause and what you really don't need is to worry about possibly
immediately fatal things through the whole pregnancy. Get the amniocentesis
done right away so that you can rule out (or deal with) these possibilities right away.
I should include here a word of warning about what an amnio can and can't tell you.
It can rule out maternal infections such as toxoplasmosis (that's the one you get from
cleaning out the cat boxes). It can rule out most chromosomal abnormalities and you'll
know definitively whether you have a boy or a girl. Finally it can detect
abnormal levels of alpha-fetoprotein which could indicate that part of the baby's internal
organs are being exposed to the amniotic fluid, such as in spina bifida.
There are a few things that it can miss
however. The most notable is that it can't detect X-Linked Aqueductal Stenosis.
If you suspect that this might be the problem, there is a separate test for it.
You have to specifically request an L1CAM gene test. This test is problematic however in that
it takes about 10 weeks to come back from the lab and it is not 100% accurate (I can't remember the
percentage anymore and I can't seem to find a reference on the web). The test is also very expensive and is
not covered by most insurance. We opted not to bother since it would be more risk in another
amnio, we'd worry for 10 weeks about it and it still wouldn't give us a 100% answer.
Get the FISH - FISH is an acronym for Fluorescence In Situ Hybridization.
This lovely long set of useless words is all about getting some of your amnio results faster.
A full amnio takes 7 to 14 days to come back and they are some of the longest days
of your life. The FISH test returns in one to two days and
is used to make certain that there are no extra chromosomes
where there shouldn't be. Normal chromosomes come in pairs, one from the mother and
one from the father. If you get an extra one you have one of the trisomy conditions
(as shown above). These types of defects account for nearly 95% of all chromosomal
abnormalities. It's not the full set of results, but it can rule out some of the biggies
early in the process. Our insurance covered the FISH because of the abnormal ultrasound,
but yours may not so I'd check into it, it's not cheap.
Get a fetal MRI done - If the amnio comes back clean and you don't therefore know
the exact cause yet, get a fetal MRI done. Even in our little podunk town in southwest
Virginia we have an imaging center that can do a fetal MRI. Your child's hydrocephalus was most
likely diagnosed during an ultrasound. Ultrasounds are great for looking at bones and fluid,
but they can't do much with soft tissue and the hydrocephalus is most likely a soft tissue problem
(unless there is a tumor or such). In our case the MRI was able to see that there was no
visible aqueduct so there was no way for the fluid to drain. You must keep in
mind however, that a fetal brain is a very small thing and once the pressure
has started to build all of the tissue gets squished so some of the smaller
structures such as the corpus callosum are very difficult to see. It may not
be possible to tell the difference between something that is not present and something
that is squished. However it can give so much more detail than an ultrasound that
even if it can't tell you the exact cause, it can probably serve to exclude certain
others.
Get yourself a really good doctor - This is subjective of course, but it is
very important. Our original OB immediately turned us over to a high risk fetal specialist as soon as
the diagnosis was made. This was fine with us, that's why they have specialists.
We were fine with our high risk guy until he started getting very vague about outcomes and
flip-flopped on delivery dates until we were frustrated and confused. This is at a hospital with
a level III NICU and excellent neonatal care. (Read our story for
more details).
We then went to a regional hospital at
a mid-size university and that was a step up. We got some better answers (we understood that
no one was going to tell us that the problem wasn't there, we just needed someone to be able
to explain it to us in terms we could understand and to be able to come up with a plan). We
were better there, but shortly after we found ourselves at Duke University Medical Center
because of the cord blood treatments mentioned above. What a difference to be in a world class
facility. The whole attitude was much different in terms of being aggressive about getting the
shunt in early and trying even experimental (although low risk) procedures to at least try and
help the baby.
There are probably a lot of local/regional hospitals with great care, even
for high risk babies, but in my book you should just start out by going to one of the best.
It depends on where you live of course, but places like Duke, Vanderbilt, Children's Hospital
of Philadelphia, UCSF Children's Hospital and those sorts are places are the place to start, not
the place to end up. After your first conversation with them you'll know why.
In our case even phone
calls with them produced more information than we were getting locally. They know of more
tests and they have a lot more experience with actual cases. Our doctors here were very
kind, but they just didn't compare.
Wait - Now that you have the results of the ultrasound, amnio and MRI, you pretty
much know everything there is to know. Depending on the type and whether or not the
blockage is complete or partial, you will be able to watch the condition progress throughout
the pregnancy but you aren't going to be able to do a thing about it. As a result this is one
of the most frustrating diagnoses out there.
What does this mean for my baby?
This is the hardest one of all to predict and it is the one that a parent cares about the most.
There are a few things to realize here that can help you keep you on the right path. The first
is that as I mentioned above, hydrocephalus is an end result. There are many causes with vastly
different ranges of outcomes. Unfortunately all of these causes have been thrown under the
same umbrella with the diagnosis of "hydrocephalus". As a result all too often when you
ask a perinatologist or other OB specialist about what the outcome is likely to be, you
will get the grimmest picture possible. When you have Trisomy 13, aqueductal stenosis and
late term IVH's being thrown into the same group, it's easy for the certainty of the poor outcome
with Trisomy 13 to overshadow the possibility of better outcomes with the other types.
What you will need to do as a parent is to follow the steps I gave above in the "What do
we do now" section. Until you have the answers to whether or not there are chromosomal problems
and until you can at least narrow down the cause, you cannot even begin your search for possible
outcomes. The results from those tests are vital to kicking the unapplicable causes out
from under the umbrella so that you can just work with the causes that actually apply to your case.
Problems with the cerebellum can cause different kinds of issues than the problems with the third
ventricle. When chromosomal abnormalities are found, there are generally a reasonably well known set
of issues that can come with those abnormalities.
Unfortunately even once you have all of your test results in hand, you will realize that
the real answer is that no one will be able to tell you exactly what will happen with your baby
unless you are facing a chromosomal abnormality that is severe enough to have a fairly
predictable outcome. The brain is a strange thing
and it is pretty much impossible to tell exactly what the outcome is going to be. In our
case the tests showed aqueductal stenosis with no chromosomal abnormalities. After hearing many
wildly ranging sets of possible outcomes for this type, our neurosurgeon at Duke finally
said it to us in a way that we could put our heads around. During the pregnancy
he said that at that point there is absolutely no way to tell if the outcome will be good or
bad. He has seen babies whose ultrasounds looked just as grim as ours turn out just fine. He has
also seen the cases with the same or better ultrasound presentations
turn out poorly with little function. The whole point is that the ultrasounds
tell you nothing other than the fact that the fluid is not draining. You can see the brain tissue
being compressed against the side of skull, but you cannot in any way tell how much damage has been
done.
Brain tissue is much like a sponge in that it can compress and expand as the pressure changes.
The key is that once the shunt is put in and the pressure is relieved you can start to watch
how much the brain tissue expands. If it expands to something nearing normal volume then there
is an 80% chance of normal or near normal brain function. If the tissue has been severely damaged
and does not expand, then the outcome will be severe. In some kids the brain just squishes and
expands with no problem and in others the squishing does a lot of damage. There is no way to know
in which category your child will be until the shunt is placed.
This doesn't make it any easier to handle the uncertainty
and for those who might choose to terminate a pregnancy it
gives you very little to work with to make a decision.
It does, however, explain in no uncertain terms what you are dealing with.
The other thing to realize is that hydrocephalus is a long term problem. Shunting doesn't "cure" the
the problem, it just manages it. Shunts have to be checked throughout your child's life as they
can get infected, clogged or malfunction in other ways. Some kids get one shunt put in and it
lasts them for years and years before they outgrow it and need a new one. Others seem to have
infection after infection and just can't seem to get it to work. As with everything else with
hydrocephalus, there is no way to know which category your child will fall into.
Legal Disclaimer: While every effort has been made to make certain that the information contained in this website is accurate, it must be remembered that the content is managed by a parent, not by a doctor. Information contained here is for general support purposes only and is no substitute for the care of a physician.